
The four kinds of statin intolerance
Statin intolerance is a spectrum, not a binary. The categories matter because they suggest different management paths:
- True statin intolerance — confirmed reproducible symptoms (or biochemical signal — significantly elevated CK) on rechallenge with two or more different statins, including at least one at the lowest possible dose. Affects roughly 2-5% of patients.
- Apparent statin intolerance / nocebo effect — symptoms attributed to the statin that do not recur on double-blind rechallenge. The literature suggests this accounts for a substantial fraction of reported statin intolerance.
- Drug-drug interaction-related intolerance — symptoms appear when a statin is combined with a specific interacting medication (certain antibiotics, some antifungals, grapefruit juice in large amounts for CYP3A4-metabolized statins). Resolves by adjusting one of the two.
- Dose-related intolerance — high doses cause symptoms but lower doses or alternate-day dosing does not. Common.
The science of the nocebo effect
The data here is well-established and worth taking seriously. The SAMSON trial (Howard et al, 2021) is the cleanest example: it enrolled 60 patients who had stopped statins because of side effects, then put each through 12 one-month periods cycling through atorvastatin 20 mg, identical-looking placebo, and no treatment. Patients tracked their symptoms daily on a phone app without knowing which they were taking.
The result: symptom severity on placebo months was 90% of the severity on statin months. The symptoms were real, but they were not specifically caused by the statin. Earlier studies including the StatinWISE trial showed similar patterns.
The clinical implication is not "ignore patient complaints" — the symptoms are real and disruptive. It is that the path to resolution often is not just "stop the statin permanently." A structured rechallenge, sometimes with placebo runs, identifies which patients truly cannot tolerate a statin and which can with a different formulation, dose, or schedule.
A structured intolerance evaluation, step by step
Step 1 — Confirm what's happening
Detailed history of which statin(s) tried, at what dose, for how long, what symptoms developed and when. Check for interacting medications, recent illnesses, vitamin D status (deficiency contributes to muscle symptoms), thyroid status, and other explanations for the symptoms.
Step 2 — Baseline labs
CK (creatine kinase) for muscle damage signal, liver enzymes, TSH, vitamin D, basic metabolic panel. These rule in or out medical contributors to the symptoms.
Step 3 — Structured rechallenge
The standard approach:
- Wait until the original symptoms have resolved (often 4-8 weeks off the statin).
- Restart at a lower dose of the same statin, OR switch to a hydrophilic statin (rosuvastatin or pravastatin) at low dose.
- If symptoms recur quickly, try alternate-day dosing or weekly dosing of a long half-life statin like rosuvastatin.
- If multiple statins fail, switch to a non-statin agent for LDL/apoB lowering.
The literature shows that about 70-80% of patients who report intolerance to one statin successfully tolerate either a different statin, a lower dose, or an alternate-day schedule of the same statin.
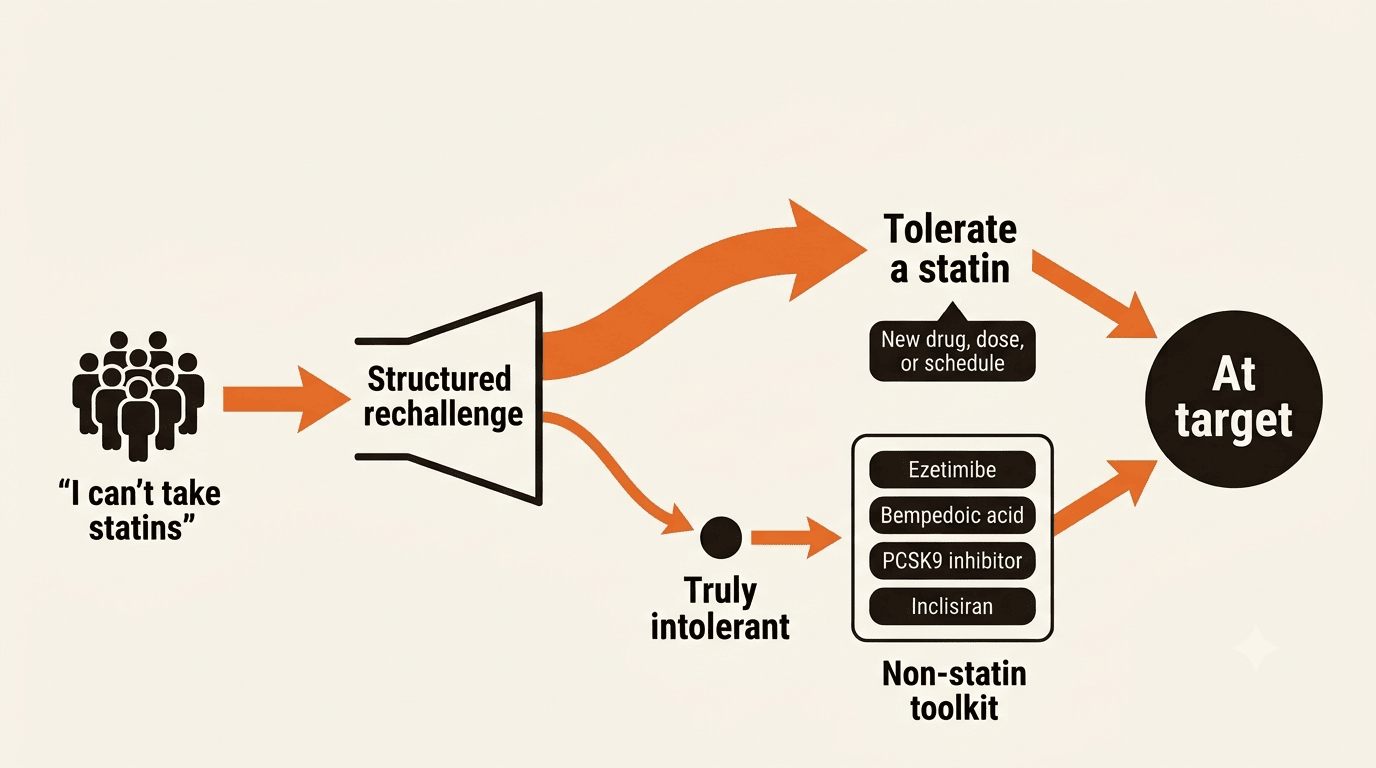
Step 4 — If true intolerance is confirmed: non-statin therapy
Modern lipid management has the tools to reach target without a statin in patients with confirmed true intolerance:
- Ezetimibe — oral, well-tolerated, reduces LDL by 15-25% as monotherapy.
- Bempedoic acid — statin-independent oral agent; reduces LDL by 15-20%.
- PCSK9 inhibitors (evolocumab, alirocumab) — injectable monoclonal antibodies; reduce LDL by 50-60%.
- Inclisiran — twice-yearly injectable siRNA; equivalent lowering to the antibodies with a much simpler dosing schedule.
Combination of ezetimibe + a PCSK9 inhibitor or inclisiran can achieve LDL lowering similar to a high-intensity statin, with no statin required.
Managing statin intolerance by video
Statin-intolerance management is a good fit for virtual care because the workflow is structured: history-taking, lab review, medication change, follow-up. Typical sequence:
- First visit by video. Detailed history, review prior labs, plan the rechallenge or the non-statin regimen if rechallenge has already failed.
- Labs drawn locally. Baseline CK, liver, vitamin D, lipids.
- Trial period. Whichever regimen we've designed, with patient-reported symptom tracking.
- Follow-up visit by video at 6-8 weeks. Reassess, repeat labs, decide whether the trial succeeded or move to the next option.
- Iterate until LDL/apoB target is achieved with tolerable therapy. Usually 2-4 cycles.
There is almost always a path forward
Statin intolerance is real but commonly overcalled. The cost of permanently stopping statins after a single side effect — without structured rechallenge or alternative-therapy plan — is years of uncovered cardiovascular risk. A systematic evaluation usually finds a path forward: a different statin, a lower dose, a different schedule, or a non-statin regimen that hits target.
See also Advanced Lipid Management for the full modern lipid toolkit, and Longevity Cardiology for the broader evidence-based prevention frame.