
The limits of a basic lipid panel
Most adults have had a basic lipid panel at some point — total cholesterol, LDL, HDL, triglycerides. That panel is fine as a screening test. It is not enough for clinical decisions in the patients who matter most: high-risk primary prevention, secondary prevention after an event, familial hypercholesterolemia, and anyone with discordant cholesterol-and-particle numbers.
Advanced lipid management adds the tests that resolve those decisions, and a treatment approach that uses the full modern therapeutic toolkit — not just whichever statin happens to be cheapest.
The diagnostic side — what we test
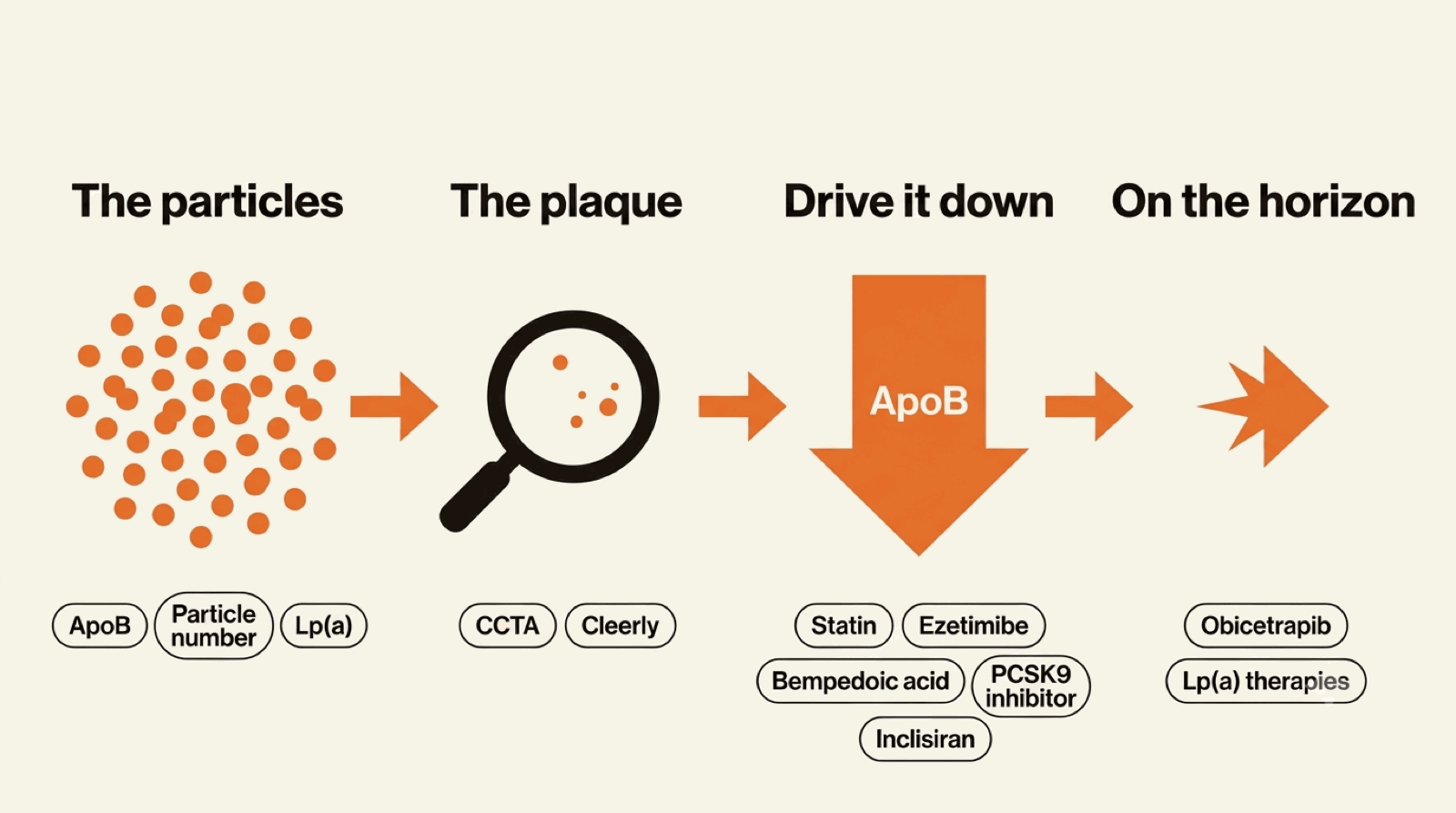
Apolipoprotein B (apoB)
The direct count of atherogenic particles in your blood. The target depends on your overall risk: roughly <90 mg/dL for primary prevention, <80 for elevated-risk patients, and <65–70 for secondary prevention.
Lipoprotein(a) — Lp(a)
One-time blood test that identifies whether you carry an elevated Lp(a). If yes, the rest of the plan is intensified accordingly. If no, that is also useful — you've ruled out a significant genetic risk factor.
Lipoprotein-particle number / size (NMR or ion-mobility)
When apoB and LDL tell different stories, lipoprotein-particle testing characterizes the discordance. Most often used for patients with metabolic syndrome, insulin resistance, or significantly elevated triglycerides.
Genetic testing for familial hypercholesterolemia (FH)
For patients with personal or family history suggesting FH — very high LDL from a young age, premature heart disease in first-degree relatives. A confirmed FH diagnosis changes both treatment intensity and family screening.
Coronary imaging — seeing the plaque, not just the particles
Labs measure how much atherogenic particle burden is circulating; imaging shows what it has already built in your arteries. The two answer different questions, and for many patients it is the imaging result that sets how hard we treat. We do not just order labs.
A coronary calcium score (CAC) is a quick, low-radiation CT that quantifies established calcified plaque. A score of zero is genuinely reassuring; any positive score is proof of established atherosclerosis, and it usually pulls the apoB and LDL targets lower and the urgency higher. CT coronary angiography (CCTA), with or without an AI-quantified overlay such as Cleerly, goes further: it images the artery wall directly, including the soft, non-calcified plaque a calcium score cannot see, and characterizes how much and what kind.
The principle that ties it together: a positive scan changes the target. Two patients with an identical LDL are not in the same place if one has a calcium score of zero and the other has soft plaque on a CCTA — the second needs a lower apoB, driven down harder and sooner. Deciding when a scan will actually change the plan, and reading the result correctly when it does, is covered in which heart test, when.
The therapeutic side — what we treat with
Statins, used correctly
Still the foundation. The right approach is the right statin and dose for your target, with follow-up labs to confirm we've hit the number. Many patients are on a low-dose statin that came from a starter prescription years ago and was never titrated to target.
Ezetimibe
Cheap, well-tolerated, additive to statin therapy with a known cardiovascular outcomes benefit. Underused in routine practice. Often the first add-on when statin alone doesn't reach apoB target.
PCSK9 inhibitors (evolocumab, alirocumab)
Injectable monoclonal antibodies that lower LDL and apoB by an additional 50–60% on top of statin therapy. Outcome trials show clear cardiovascular benefit. Coverage is broader than most patients realize; we handle the prior authorization.
Inclisiran
Twice-yearly injectable siRNA that silences hepatic PCSK9 production. Equivalent LDL lowering to the antibodies, with a dramatically simpler dosing schedule.
Bempedoic acid
Oral, statin-independent, useful in statin-intolerant patients and as an add-on for patients who can't reach target on statin alone.
Icosapent ethyl, for patients with elevated triglycerides on statin
Evidence-based add-on with a cardiovascular outcomes benefit in high-risk patients whose triglycerides remain elevated despite statin therapy.
If you already have advanced lab results in hand
A growing number of patients arrive with results from a consumer-ordered advanced lab panel — Function Health, InsideTracker, Levels, or a direct-to-consumer order through Quest or LabCorp. These panels typically include the metrics that matter most: apoB, lipoprotein(a), particle number, hs-CRP, homocysteine, and sometimes Lp-PLA2 or remnant cholesterol. The numbers are real and they matter — but the report does not tell you what to do with them.
That is exactly the conversation we are built for. Bring your results to the first visit and we will work through what each number actually means for your risk picture, what additional testing is indicated, and what treatment plan — if any — gets you to target. You do not need to re-order anything to start; if a panel is missing a marker we want, we will add it on the first round of labs rather than duplicate what you have.
The program, step by step
- First visit (30 min). Review your history, family history, prior labs, current medications, lifestyle, and goals. Order the advanced lipid panel + any other tests indicated.
- Labs drawn near home. Quest, LabCorp, or a local lab — wherever is most convenient. Results arrive electronically.
- Follow-up visit (15–30 min). Walk through the results together. Build the treatment plan: target, regimen, whether add-on therapy is needed.
- Titration visits as needed. Labs at 8–12 weeks after each change to confirm response. Most patients reach target in two to four titration cycles.
- Ongoing. Annual labs and one follow-up visit per year is typical for stable patients.
The most evidence-based intervention in cardiology
Lipid management is the single most heavily evidence-based intervention in adult cardiology. Done with the full modern toolkit, targeted to apoB, and tuned to the individual's true risk, it is also one of the highest-leverage things you can do for your long-term cardiovascular outcomes. This program is designed to bring that level of care within reach of a virtual visit.