
Heart disease builds for decades before it shows
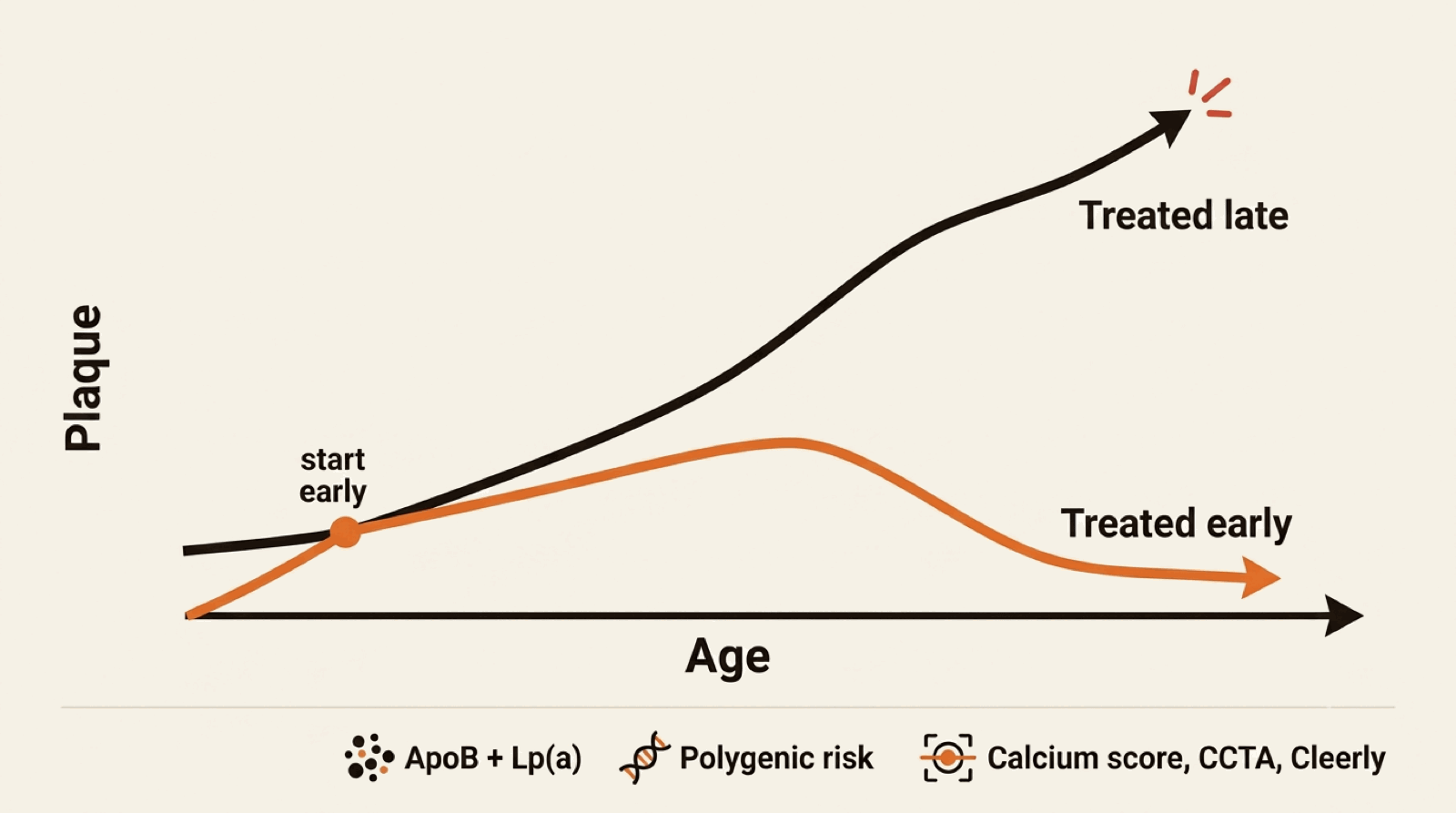
Atherosclerosis — the buildup of plaque in coronary arteries — is the disease behind most heart attacks and a significant fraction of strokes and heart failure cases. It is also one of the slowest diseases in medicine: the plaque that causes a heart attack at 60 has been building since the patient was in their 30s. That is the opportunity. The window for intervention is decades wide, but only if you measure the right things and act on them early.
Longevity cardiology is the structured approach to using that window: identify each individual's true cardiovascular risk earlier and more precisely than the standard primary-care calculation does, and treat that risk before it becomes disease. This is what the evidence supports — and increasingly what specialty cardiology societies recommend — but it is not what most patients get from a once-a-year primary-care visit.
The advanced workup: what standard care leaves out
Apolipoprotein B (apoB)
LDL cholesterol is the input most people know. apoB is the more accurate one — it directly counts the atherogenic particles in your bloodstream. In about a third of patients, the apoB and LDL numbers tell meaningfully different stories, and the apoB number is the one that better predicts events.
Lipoprotein(a) — Lp(a)
A genetically determined risk factor most patients have never had measured. About 20% of the population has an elevated Lp(a), which confers significantly higher lifetime risk of heart attack and aortic valve disease independent of cholesterol numbers. It is a one-time blood test. Knowing your Lp(a) status changes how aggressively we treat everything else, and new Lp(a)-lowering therapies are in late-stage trials.
Coronary artery calcium (CAC) scoring
A low-radiation CT scan that directly visualizes plaque calcification in your coronary arteries. A zero score in your 50s is one of the strongest reassurance signals in cardiology. A non-zero score restratifies your risk in a way no blood test can match, and it is the single piece of information that most often changes our treatment plan.
CT angiography and AI plaque analysis (CCTA, Cleerly)
When a calcium score raises questions or a fuller picture is warranted, coronary CT angiography images the arteries directly — including the soft, non-calcified plaque a calcium score cannot see. AI-based analysis such as Cleerly quantifies the amount, type, and distribution of that plaque, and can track whether it is stabilizing or progressing over time. We review whether it is the right test for you, order it at a center near you, and walk through the result together. More: calcium score, CCTA, and Cleerly compared.
Polygenic risk scoring
A genetic risk score for coronary artery disease — a single one-time test that summarizes the combined effect of hundreds of common variants. It identifies people whose inherited risk diverges from their conventional risk factors. The data supporting clinical use of polygenic risk scores in cardiology has matured significantly in the last few years.
Inflammation markers
High-sensitivity CRP and, when indicated, more specific markers. Persistent inflammation is an independent driver of cardiovascular events, and new anti-inflammatory therapies are FDA-approved for secondary prevention.
From measurement to a treatment plan
Measurement only matters if it changes what you do. The reason to go deeper is that it lets us treat earlier and more precisely than the standard once-a-year approach — while the window is still open.
Lower the atherogenic particles, and start early
The strongest lever in cardiovascular prevention is lowering apoB and LDL and keeping them low over years — and the earlier that starts, the more disease is prevented. Statins are the foundation but no longer the whole story: ezetimibe, bempedoic acid, PCSK9 inhibitors, and inclisiran extend how far and how reliably the number comes down, including for patients who cannot tolerate statins. The higher your risk — from an elevated Lp(a), a positive calcium score, or your genetics — the more aggressive the target. More: the modern cholesterol toolkit.
Treat the whole risk profile, not one number
Blood pressure, metabolic health, and inflammation when it is present are all part of the plan. When Lp(a) is high, we intensify every other lever, since Lp(a) itself has no approved specific therapy yet — though several are in late-stage trials.
Confirm the plan is working
A risk number is abstract; a trend is not. Where imaging is part of the plan, repeat assessment can show whether plaque is stabilizing — turning treatment into something you can actually watch respond.
On the horizon
The next few years of lipid therapy are genuinely exciting, and part of the value of a cardiologist who follows the field closely is knowing what is coming and when it might change your plan. Obicetrapib, an oral drug in Phase III trials, lowers both LDL and Lp(a). Several Lp(a)-specific therapies — antisense and siRNA drugs — are in Phase III outcome trials, the first real prospect of lowering a risk factor that has never had a targeted treatment. We track these so the plan we build today already accounts for what is coming into view. Read more: Lp(a) therapies, now and soon.
Every test has to earn its place
It is not a "wellness" panel or a vitamin-and-supplement consultation. It is also not concierge medicine in the membership-fee sense. Every test we order has a specific evidence-based reason it changes the plan. We do not order what will not change a decision.
The Deo Medical approach
What patients come to us for is not one test or one drug. It is a cardiologist who orders the tests that actually change the plan, prescribes the newer therapies when they fit, keeps up with what is still in trials, reads the evidence as it evolves, and — hardest of all — integrates advanced lipids, imaging, and genetics into a single coherent plan rather than a pile of unconnected results.
Our cardiologists' clinical training is in cardiology — including the interventional, imaging, and outpatient sides — at Harvard-affiliated institutions. His research background is in applying AI and genomics to cardiology, including coauthoring some of the foundational work on machine-learning interpretation of echocardiograms. That dual background is why this program is structured around the evidence base and the technology that actually moves outcomes — not the version that just looks impressive.