
Atrial fibrillation, in plain terms
Normally, each heartbeat starts in a tiny patch of pacemaker tissue in the right atrium and travels through the heart in a coordinated sequence. In atrial fibrillation, the atria stop beating in that coordinated way and instead quiver chaotically — electrical signals fire from many points at once. The ventricles still beat, but in an irregular and often fast pattern dictated by which atrial signals happen to get through.
Two consequences follow from that: (1) the irregular, often-rapid rhythm can cause symptoms — palpitations, breathlessness, fatigue, reduced exercise tolerance, sometimes lightheadedness; and (2) blood can stagnate in the atria, particularly in a structure called the left atrial appendage, which raises the risk of a clot forming and being thrown to the brain as a stroke. Almost all of modern AFib management is about addressing one or both of those.
The types of AFib
Cardiologists describe AFib by its time course, because the right treatment often differs by pattern:
- Paroxysmal AFib — episodes that start and stop on their own, typically lasting from minutes to days. Often the earliest pattern.
- Persistent AFib — episodes that last more than a week or require intervention (cardioversion, antiarrhythmic medication) to convert back to normal rhythm.
- Long-standing persistent AFib — continuous AFib for more than 12 months, with a strategy still aimed at restoring sinus rhythm.
- Permanent AFib — a clinical decision (made together with the patient) to accept the rhythm and focus on rate and stroke-risk management rather than restoring sinus rhythm.
The pattern can change over time — paroxysmal AFib often progresses to persistent if left untreated, which is part of the rationale for earlier intervention now than was standard a decade ago.
Diagnosing AFib
The diagnosis is electrical — a recording of the heart rhythm showing the characteristic irregularity. The recording can come from several places:
The 12-lead ECG
The traditional gold standard. If you can be ECG'd while in AFib, the diagnosis is straightforward. The problem is that paroxysmal AFib may not be present during a scheduled visit, which is where monitors come in.
Rhythm monitors
Several formats, picked to match how often the episodes happen:
- 24- to 48-hour Holter monitor for very frequent symptoms.
- 1- to 2-week patch monitor for episodes a few times a week.
- 30-day event monitor for less frequent episodes.
- Implantable loop recorder for rare episodes where the cardiac question is important enough to warrant months-to-years of continuous monitoring.
Most monitors are ordered to ship to your home; you wear them for the prescribed period and they upload data electronically for the cardiologist to review.
Smartwatch and personal ECG devices
This is one of the biggest changes in the field. Apple Watch, Fitbit, Kardia, and Withings devices can now detect irregular rhythms with reasonable accuracy and produce a short ECG tracing you can email to your cardiologist. The 2018 Apple Heart Study established that consumer-grade detection has clinical value, and follow-on guidelines have integrated wearables into AFib screening and follow-up. If you have one, a tracing captured during symptoms is a useful clue that can point us to the right test — but a single-lead reading screens for AFib rather than diagnosing it; the diagnosis is confirmed with a 12-lead ECG or an ambulatory monitor.
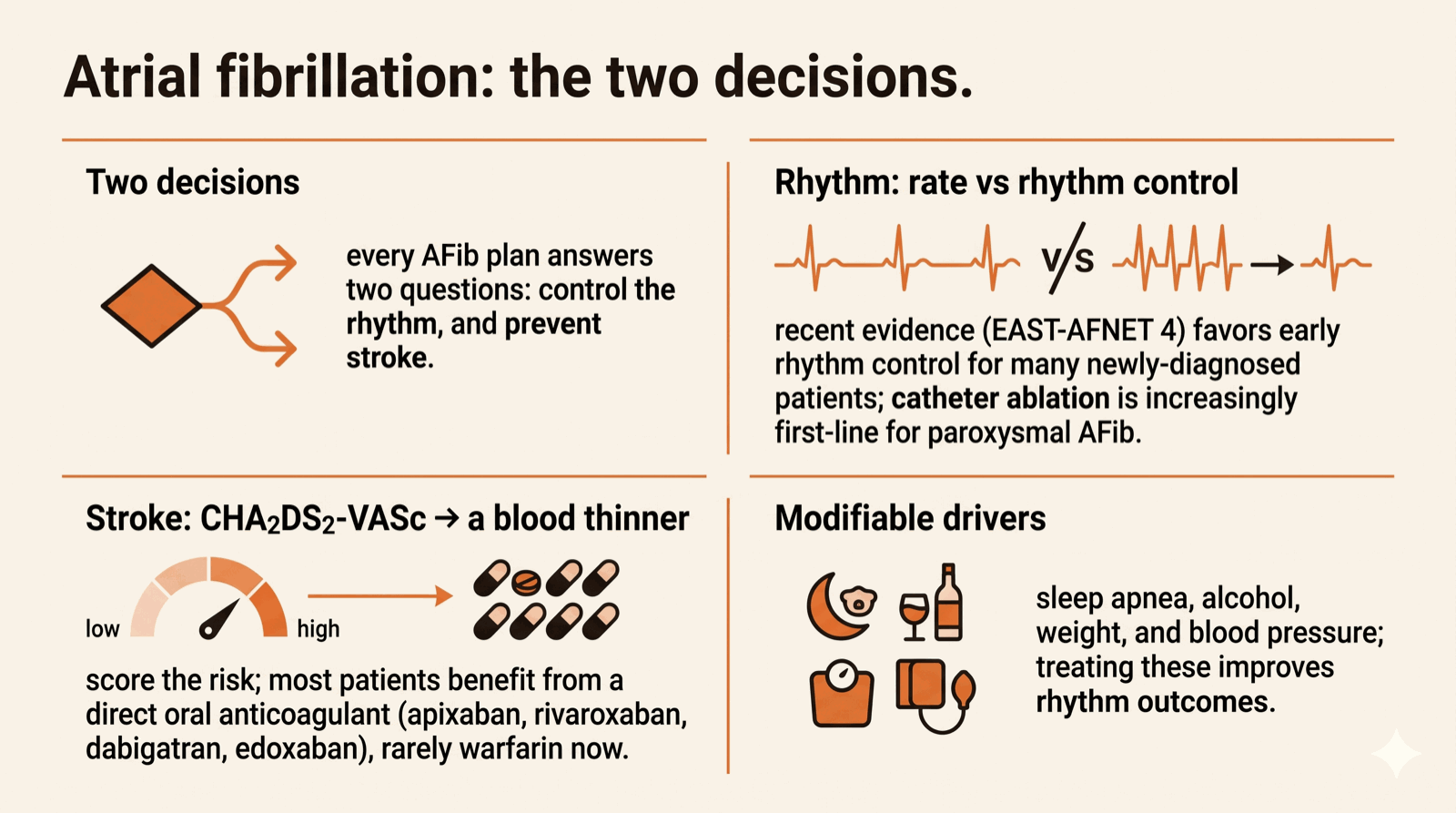
The two decisions in AFib management
Two decisions, made together — and reassessed over time:
Decision 1 — what to do about the rhythm
Rate control uses medications to slow the ventricular response so the heart pumps at a reasonable rate even if the underlying rhythm is AFib. The mainstays are beta blockers (metoprolol, bisoprolol, carvedilol), calcium channel blockers (diltiazem, verapamil), and occasionally digoxin. Goal heart rate is typically under 110 bpm at rest in mostly-asymptomatic patients, sometimes lower in patients with symptoms or reduced ventricular function.
Rhythm control aims to restore and maintain normal sinus rhythm. Options include antiarrhythmic medications (flecainide, propafenone, sotalol, dofetilide, amiodarone, dronedarone — each with its own indications and contraindications), direct-current cardioversion (a controlled electrical shock to restore sinus rhythm), and catheter ablation (pulmonary-vein isolation, increasingly first-line for symptomatic paroxysmal AFib).
The choice between rate and rhythm control has shifted recently. The EAST-AFNET 4 trial showed that early rhythm control — within the first year of AFib diagnosis — reduces cardiovascular events compared with rate control alone for many patients. The result was that "rate control is good enough for almost everyone" is no longer the default position; early rhythm control deserves consideration for most newly-diagnosed symptomatic patients.
Decision 2 — what to do about the stroke risk
The CHA₂DS₂-VASc score is the standard tool for estimating stroke risk in AFib. It assigns points for:
- Congestive heart failure (1 point)
- Hypertension (1 point)
- Age 65–74 (1 point) or 75+ (2 points)
- Diabetes (1 point)
- Prior stroke or TIA (2 points)
- Vascular disease — prior MI, peripheral artery disease, aortic plaque (1 point)
- Sex category — female (1 point)
Anticoagulation is generally recommended for men with a score of 2+ and women with a score of 3+; in lower scores the decision is individualized.
Modern anticoagulation is almost always with a direct oral anticoagulant (DOAC) — apixaban (Eliquis), rivaroxaban (Xarelto), dabigatran (Pradaxa), or edoxaban (Savaysa). DOACs reduce stroke risk dramatically, have lower bleeding rates than warfarin in most populations, do not require INR monitoring, and have fewer food/drug interactions. Warfarin remains first-line in patients with mechanical heart valves and a few other specific scenarios.
Lifestyle factors that matter for AFib
AFib is not just an electrical disease — it has structural and metabolic drivers that respond to lifestyle modification:
- Sleep apnea. Untreated obstructive sleep apnea is a major driver of AFib recurrence and progression. Screening and treatment (often CPAP) substantially improves rhythm outcomes.
- Alcohol. Even modest regular alcohol intake (more than 1–2 drinks per day) increases AFib risk and triggers episodes. The LEGACY and AFFIRM trials showed that reducing or eliminating alcohol improves AFib outcomes.
- Weight. Sustained weight loss in overweight patients reduces AFib burden — sometimes dramatically.
- Blood pressure. Tight BP control reduces progression and recurrence.
- Exercise. Regular moderate exercise improves outcomes; extremely high-intensity endurance training in some athletes paradoxically increases AFib risk, but this is uncommon.
Managing AFib by video
AFib management is among the best fits for the virtual model. The workflow:
- First visit by video. Detailed history, review of any prior records, ECGs, monitor data, and smartwatch tracings. Initial classification (paroxysmal vs persistent), risk stratification (CHA₂DS₂-VASc), and a treatment plan.
- Diagnostic workup completed locally. Labs (TSH, basic metabolic panel, lipid panel), echocardiogram, rhythm monitor as needed — all ordered to imaging centers and labs near home. Sleep-apnea screening if indicated.
- Follow-up visit to interpret results and finalize the plan. Anticoagulation decision, rate vs rhythm control strategy, and lifestyle plan.
- Longitudinal management. Visits every 3–6 months depending on stability, with smartwatch tracings and monitor data reviewed between visits as needed. Medication titration handled by video. Catheter ablation or electrical cardioversion coordinated with local cardiology when indicated.
Getting in front of AFib is worth it
Atrial fibrillation has moved in the last decade from "manage the rate and accept the rhythm" to "consider early rhythm control, optimize the modifiable drivers, and protect against stroke aggressively." The diagnostic tools — including the one on your wrist — are excellent, the medications are better than they have ever been, and the procedural options have matured. AFib done well is a manageable chronic condition; AFib left alone is the leading preventable cause of stroke in adults. Getting in front of it is worth doing.