The new cholesterol guidelines: Lp(a), ApoB, and treating at lower thresholds
The 2026 dyslipidemia guidelines from the American College of Cardiology and American Heart Association are out. They shift several things meaningfully. Most patients will not hear about them from their primary care doctor for a year or more. Guideline updates take time to propagate. Here is what is different, what it means for you, and the two tests (Lp(a) and ApoB) you may need to ask for by name.
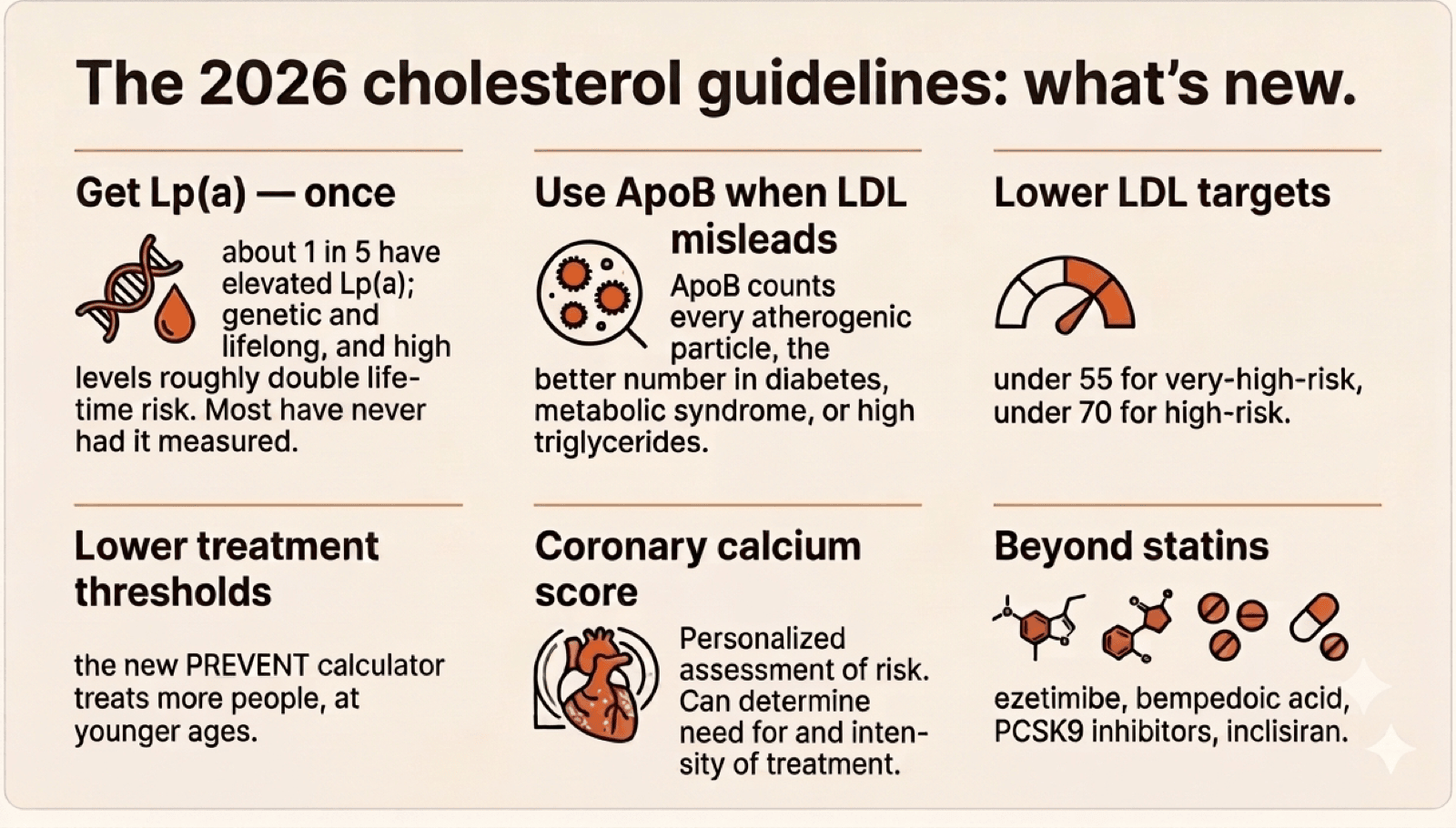
The biggest change: lower treatment thresholds
For most of the last decade, cardiologists used the Pooled Cohort Equations to estimate your 10-year risk of a heart attack or stroke. The new guidelines use a calculator called PREVENT, which incorporates more inputs — kidney function, optionally social factors and HbA1c — and importantly, removes race. The old equations gave different risk estimates by race, which has aged poorly.
PREVENT generally produces lower 10-year risk numbers than the old calculator for the same patient. The guideline writers responded by lowering the treatment thresholds:
| Risk category | Old (Pooled Cohort) | New (PREVENT) |
|---|---|---|
| Low | <5% | <3% |
| Borderline | 5–7.5% | 3–5% |
| Intermediate | 7.5–20% | 5–10% |
| High | ≥20% | ≥10% |
Practical implication: more patients are treatment candidates than were before, and at younger ages. A common scenario: 52-year-old man, exercises regularly, no diabetes, no high blood pressure, LDL 135 mg/dL, PREVENT 10-year risk of 3.8%. Old thinking might have left him on lifestyle advice. New guidelines say offer a moderate-intensity statin. If he is reluctant, a coronary calcium scan is reasonable, and if it shows any plaque, treat.
LDL targets dropped
For patients with established cardiovascular disease, LDL targets are now more aggressive:
- Very high-risk ASCVD (prior heart attack or stroke with high-risk features): LDL-C target <55 mg/dL, non-HDL-C <85 mg/dL.
- ASCVD, not very high risk: LDL-C <70 mg/dL, non-HDL-C <100 mg/dL.
- High primary-prevention risk (PREVENT 10-year ≥10%): LDL-C <70 mg/dL.
- Primary prevention with risk enhancers: typically LDL-C <100 mg/dL.
A scenario where this matters: patient had a heart attack five years ago, is on a statin, LDL is 85 mg/dL, feels fine, the prior target was <70 and "close enough" was OK. New target is <55. That is a real treatment intensification conversation.
The toolkit beyond statins
Statins are still first-line. But the menu of add-ons has grown enough that "I cannot take a statin" is no longer the end of the conversation.
| Medication | LDL lowering | When it is used |
|---|---|---|
| Ezetimibe | 15–25% | First add-on. Cheap, oral, very well tolerated. Often added before any other adjustment. |
| Bempedoic acid | 15–25% | Useful for statin-intolerant patients. Oral. Watch for gout risk and tendon issues. |
| PCSK9 inhibitors (alirocumab, evolocumab) | 50–60% | High-risk patients still above target on statin + ezetimibe; familial hypercholesterolemia. Injection every 2–4 weeks. Insurance approval requires documentation. |
| Inclisiran | ~50% | An siRNA injection every 6 months. Adherence advantage; outcomes data still maturing. |
Important practical point: in patients with established disease who are far above their LDL goal, the guidelines now urge moving quickly to combination therapy rather than incrementing slowly over years. "Wait six months and see" on a patient already in trouble is not the right call.
Statin muscle symptoms: what to do
Statin muscle complaints are common enough to deserve their own paragraph. The reality is mixed: in randomized trials, the rate of statin-attributable muscle symptoms is much lower than patient self-report. But the experience is real for many people, and dismissing it does not help anyone.
How I work through it in practice:
- Confirm the timing. Symptoms that started before the statin or with no relationship to dose changes are probably not the statin. True statin myopathy correlates with starting the drug, escalating dose, or adding an interacting medication.
- Rule out other causes. Hypothyroidism and drug interactions are common contributors; both are worth checking.
- Rechallenge intelligently. Lower dose, a different statin (pravastatin and rosuvastatin tend to be better tolerated), or alternate-day dosing. Many patients tolerate a different statin or schedule when the first attempt did not work.
- Keep LDL-lowering moving regardless. Ezetimibe and bempedoic acid together cover ~30–50% LDL lowering, close to what a moderate statin would do. PCSK9 inhibitors are the next step in high-risk patients who cannot tolerate any oral combination.
A phrase I use with patients: "We are not choosing between a statin and nothing. We are working with you to find a cholesterol-lowering plan you can actually tolerate." That is almost always achievable.
Lp(a): the genetic risk factor most patients have never had measured
Lipoprotein(a), written as Lp(a), is an inherited lipid particle that increases lifetime cardiovascular risk independently of your LDL. It is:
- Genetic and stable over your life. You inherit it. It does not change much with diet or exercise. One measurement is essentially enough for life.
- Common. About 20% of the population has elevated levels.
- Risk-multiplying. Levels above 200–250 nmol/L approximately double lifetime cardiovascular risk.
- Under-tested. Until recently, mainstream guidelines did not push for routine testing because there was no specific Lp(a)-lowering drug. That has changed: guidelines now recommend testing at least once in adulthood.
- Hereditary. If yours is high, first-degree relatives should be tested.
What you can do about a high Lp(a) today: be more aggressive about everything else. Tighter LDL goals, more willing use of PCSK9 inhibitors (which lower Lp(a) modestly), aggressive blood-pressure and smoking control. Specific Lp(a)-lowering drugs (pelacarsen, olpasiran) are in late-stage trials but not yet approved.
The test costs roughly $50–150 and most insurance covers it. It is appearing in more direct-to-consumer panels (Function Health, others). It should be a normal part of an adult lipid workup at least once. If you have never had it, ask.
ApoB: when LDL underestimates your risk
Apolipoprotein B (ApoB) counts the number of atherogenic lipoprotein particles in your blood: LDL, VLDL, IDL, and Lp(a) combined. Every one of those particles carries exactly one ApoB molecule. Standard LDL-C measures the cholesterol inside the particles, not the particle count.
For most patients those two measurements line up. For some they do not, and ApoB gives the more accurate risk picture:
- Type 2 diabetes and metabolic syndrome. These patients often carry many small, dense LDL particles. Each particle has less cholesterol in it, so LDL-C looks deceptively reasonable while ApoB (and actual risk) is high.
- Mixed dyslipidemia: high triglycerides, low HDL, with LDL that does not look that bad. Same story.
- Patients already on a statin who want a more accurate read on whether further intensification is warranted.
ApoB targets are broadly comparable to LDL-C: under 80 mg/dL for high-risk patients, under 65 mg/dL for very high-risk. It costs ~$30–60 and most insurance covers it. If your LDL looks fine but you have type 2 diabetes, metabolic syndrome, or high triglycerides, an ApoB measurement is worth getting. It often reclassifies risk and can change the conversation about treatment.
The exceptions to aggressive targets
A few groups warrant aggressive treatment even if their calculated risk is low:
- LDL-C above 190 mg/dL (often genetic, including familial hypercholesterolemia). Treat regardless of calculated risk.
- Type 1 or type 2 diabetes age 40+ (or younger with additional risk factors). Moderate-to-high intensity statin.
- Chronic kidney disease stage 3 or higher, age 40+. Moderate-to-high intensity statin.
- Strong family history of premature cardiovascular disease. Screen earlier; treat younger.
If you have any of these, the calculator number is not the whole story.
The practical takeaways
Even if you skim everything above:
- Get a current cardiovascular risk estimate. Ask your doctor to run PREVENT. The numbers and the thresholds have both moved.
- Get Lp(a) measured once. If never done, this is overdue.
- Get ApoB if your LDL looks OK but you have type 2 diabetes, metabolic syndrome, or high triglycerides. It often tells a different story.
- If you are on a statin and tolerating it, ask what your LDL goal is now versus when you started. It may have tightened.
- If you struggled with a statin in the past and stopped, know that the options today are much wider than they were 5–10 years ago.
The shorthand version: screen earlier, treat at lower thresholds, aim lower, use the broader toolkit, and do not let calculator categories be the only input.
Want a cardiologist to actually run PREVENT, order Lp(a) and ApoB, and walk through what the new targets mean for you?
Book a Video Visit