Lp(a) therapies: what we have today, and what's coming
Patients increasingly arrive at my visits having just found out their Lp(a) is elevated. They have a number on a recent lipid panel, a Facebook group's worth of context, and one question: now what. Here is the straight answer in 2026.
A quick refresher (for the patient who skipped ahead)
Lp(a) — pronounced "L-P-little-a" — is a particle in your blood that looks a lot like LDL, with an extra protein called apolipoprotein(a) wrapped around it. About one in five people have elevated Lp(a). The level you are born with is largely the level you have for life. It does not move appreciably with diet, exercise, weight loss, statins, or anything else you can buy at the grocery store.
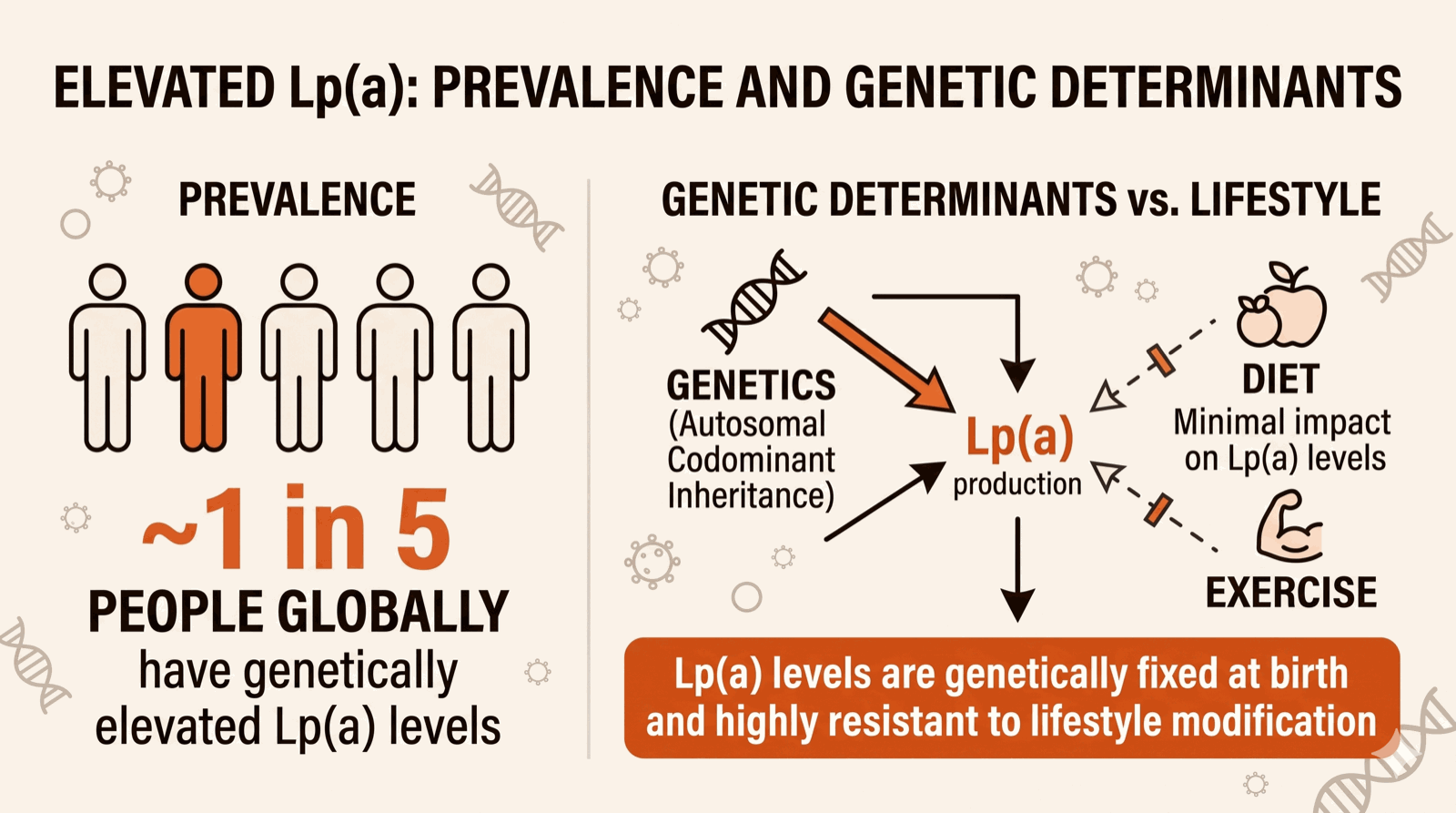
Elevated Lp(a) raises your risk of heart attack, stroke, and aortic stenosis, independent of and on top of every other risk factor. We know this from Mendelian randomization (people born with genes that produce high Lp(a) get heart attacks more often) and from large observational cohorts. It is the most common genetic risk factor for early cardiovascular disease that primary care almost never checks. That is changing slowly. If your parent or sibling had a heart attack before about 55–60, you should know your Lp(a).
Test once. The level is stable through life, so unless you are tracking response to a future Lp(a)-lowering medication, you do not need to repeat.
The tools we have today
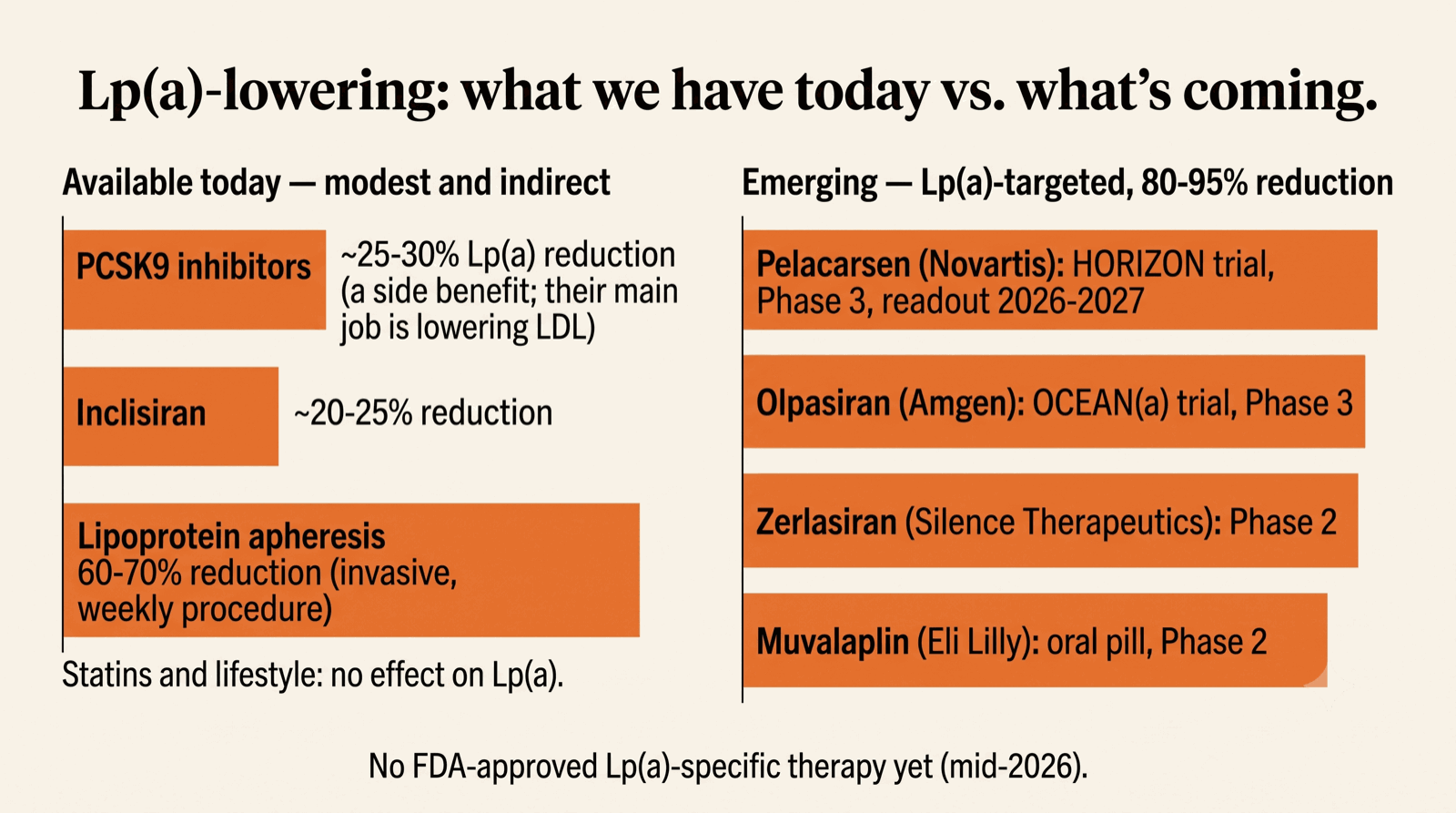
As of mid-2026 there is no FDA-approved therapy that targets Lp(a) specifically. That sentence is the source of most of the frustration patients arrive with. The medications we do have either lower Lp(a) modestly as a side effect of doing something else, or are blunt and invasive.
PCSK9 inhibitors (alirocumab/Praluent, evolocumab/Repatha) lower Lp(a) by roughly 25–30%, alongside their primary effect of dropping LDL by 50–60%. They are FDA-approved for LDL lowering and cardiovascular risk reduction, not for Lp(a) per se. In post-hoc analyses of the FOURIER trial (evolocumab) and ODYSSEY OUTCOMES (alirocumab), the benefit was larger in patients who started with the highest Lp(a). They are injectables (once every two weeks or monthly) and historically expensive, though list prices have come down meaningfully.
Inclisiran (Leqvio) is a small interfering RNA that knocks down PCSK9 production in the liver. Same downstream biology, but only two injections a year after the loading doses. It lowers Lp(a) by a similar ~20–25%, and like the antibodies it is FDA-approved for LDL, not for Lp(a).
Niacin lowers Lp(a) by roughly 25% and was used for that purpose for years. Two large outcome trials (AIM-HIGH, HPS2-THRIVE) showed no cardiovascular benefit and substantial side effects. We have largely stopped recommending it for Lp(a).
Aspirin lowers Lp(a) modestly (~10–15%) in some studies. The recent post-hoc analysis from the ASPREE trial suggested aspirin may have a primary-prevention benefit specifically in people with elevated Lp(a). This is not yet a guideline recommendation, but is one of the threads worth watching. For now I do not start aspirin for Lp(a) alone in someone without other indications, but the evidence is interesting.
Lipoprotein apheresis is the nuclear option, a weekly or biweekly procedure that filters Lp(a) out of your blood. It lowers Lp(a) by ~60–70% acutely. It works. It costs about $50,000 a year and requires showing up weekly to an apheresis center. It is reserved for patients with very high Lp(a) and established cardiovascular disease who are not controlled by other means. Most patients I see do not need it; the option exists for the small fraction who do.
The gaps that remain
Diet and lifestyle do not lower Lp(a) meaningfully. I want to be candid about this because every other lipid problem has a lifestyle lever and patients reasonably expect one here. They cut saturated fat, lose 15 pounds, exercise five days a week, and their Lp(a) does not budge. That is not their failure. The protein you make is encoded by your LPA gene; the gene does not care how you ate this month.
Statins do not lower Lp(a) either. Some studies suggest they nudge it up by a few percent. The clinical significance is unclear; the point is, do not stop your statin to "fix" your Lp(a), because the statin is doing other useful things and is not the cause of the number.
Your move today with high Lp(a)
The high-leverage move while we wait for the new drugs is aggressive control of everything else. Elevated Lp(a) is like running with a 20-pound weight vest: every other risk factor matters more for you than for someone without it. Specifically:
Drive your LDL lower than the standard target for your risk profile. If guidelines say a high-risk patient should be under 70, I usually want someone with elevated Lp(a) and high CV risk under 55, sometimes lower. The PCSK9 inhibitors and inclisiran help here, and their Lp(a) effect is a useful bonus.
Drive your blood pressure to target. Stop smoking if you smoke. Treat diabetes aggressively. Sleep. Move. Manage weight. All of the boring advice matters more for you, not less.
Get good imaging of where you actually stand. A coronary calcium score (CAC), sometimes a CT coronary angiogram if the picture is murky, tells you what your arteries look like now. Two people with the same elevated Lp(a) can have very different arterial reality at age 50 depending on how the rest of their risk profile has played out. That picture changes the conversation more than the Lp(a) number alone.
On the horizon, 2026–2028
Four drugs in late-stage development target Lp(a) directly, knocking down production of apolipoprotein(a) at the genetic or protein-assembly level. In Phase 1 and 2 trials, all four produced Lp(a) reductions of 80–95%, the kind of effect we normally only see for LDL with the most potent therapies. The question every one of them is asking is whether lowering Lp(a) by that much actually reduces cardiovascular events. That outcome question is what the Phase 3 trials are designed to answer.
Pelacarsen (Novartis) is an antisense oligonucleotide that blocks the messenger RNA for apolipoprotein(a) in the liver. The HORIZON Phase 3 trial finished enrollment of about 8,000 patients with established cardiovascular disease and elevated Lp(a). Primary outcome readout is expected in the 2026–2027 window. It is the furthest-along Lp(a) drug; the trial result will shape the field.
Olpasiran (Amgen) is a small interfering RNA (same kind of mechanism as inclisiran for PCSK9) that silences apolipoprotein(a) production. The OCEAN(a) Phase 3 trial is enrolling. Olpasiran is dosed less frequently than pelacarsen (every 12 weeks vs every 4) and in Phase 2 data produced Lp(a) reductions over 95%.
Zerlasiran (Silence Therapeutics) is another siRNA in earlier-stage trials, with similar Lp(a) knockdown.
Muvalaplin (Eli Lilly) is the interesting outlier: an oral pill that disrupts the assembly of the Lp(a) particle in the liver instead of knocking down its production. Phase 2 data showed Lp(a) reductions of 65–85% with daily dosing. If it survives Phase 3, an oral once-daily Lp(a) drug would change the practical experience for patients more than any of the injectables.
None of these are FDA-approved yet. Two important caveats. First, large reductions in Lp(a) are necessary but not sufficient. The field is waiting to see whether the cardiovascular benefit tracks. Statins and PCSK9 inhibitors both lowered LDL and reduced events proportionally; Lp(a) biology is similar but not identical, and the trials need to confirm. Second, even after approval, these drugs will be expensive, will be injectables (or pills, for muvalaplin), and will likely first be approved for secondary prevention in patients with established CV disease and very high Lp(a). Wider primary-prevention use will come later if the data support it.
Should you get tested?
Yes, if any of the following apply:
A parent, sibling, or child had a heart attack or stroke
before about age 55 (men) or 65 (women), especially without
the usual risk factors.
You yourself have had a cardiovascular event at a younger
age than expected.
Your LDL is higher than expected given your diet and family
history, or is hard to bring down with standard therapy.
You have established cardiovascular disease and the standard
risk factors are all controlled. Lp(a) explains some of the
unexplained risk.
Even without these triggers, plenty of cardiologists are now recommending a one-time Lp(a) check for any adult, on the argument that it is a stable lifelong number and the information will eventually be actionable as the new drugs come through. I largely agree.
The short version
If you have elevated Lp(a) today, the leverage is aggressive control of every other risk factor, especially LDL, and a clear-eyed picture of where you stand (calcium score or CCTA depending on the situation). The PCSK9 inhibitors and inclisiran do useful double duty. The Lp(a)-specific drugs are coming; the first outcome trial reads out in the next 12–24 months. If you are someone whose Lp(a) is dominating your risk picture, you are not stuck. You are early.
— Rahul Deo, MD, PhD
Want your Lp(a) taken seriously, with a plan to act on it?
Book a Video Visit