Cleerly, CCTA, and calcium scores: which heart test, when?
Patients ask me about Cleerly scans constantly. The marketing is everywhere: an AI-powered scan that maps the plaque in your arteries in extraordinary detail. The technology is real, the imaging is genuinely impressive, and for the right patient it can change care meaningfully. For the wrong patient, it is expensive overkill, will not change what we do, or, worse, finds something we then chase that did not need chasing.
First, three tests that get conflated
Three things get bundled together in patient conversations. Worth separating them.
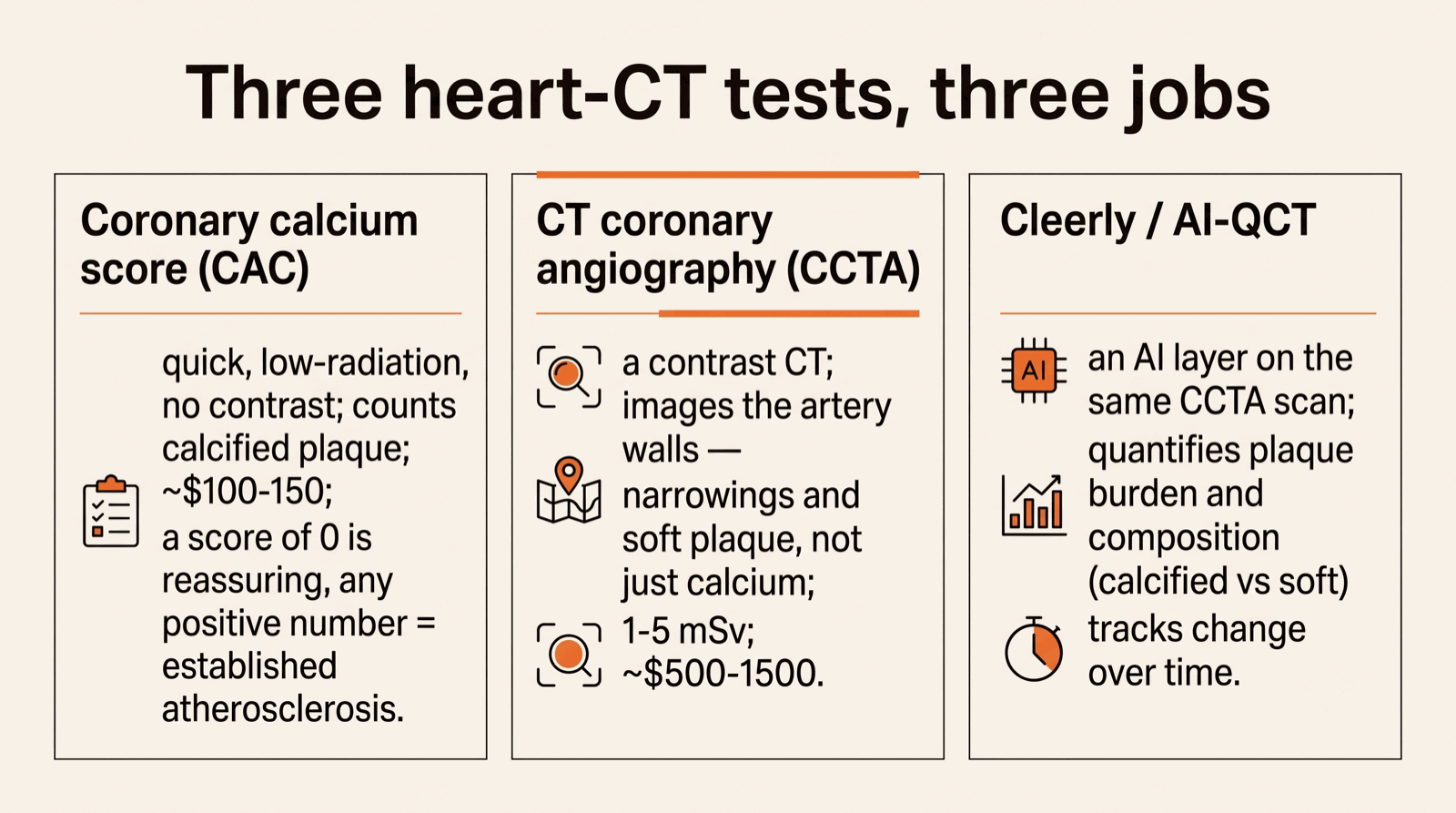
Coronary calcium score (CAC). A quick, low-radiation CT scan that counts calcium in your coronary arteries. Costs roughly $100–150. Tells you whether you have accumulated calcified plaque and roughly how much. A score of zero is good news; any positive number means you have established atherosclerosis. Has been around for decades.
CT coronary angiography (CCTA). A higher- resolution CT with contrast dye that images the actual coronary arteries, not just the calcium in them. Shows narrowings, soft plaque, the anatomy of where blockages are. Radiation is higher than a calcium score (1–5 mSv) but lower than a nuclear stress test (10–15 mSv).
Cleerly (and similar AI-QCT tools). An AI layer on top of CCTA. The scan is the same scan; what is different is that an AI quantifies plaque burden, composition (calcified, fibrous, fatty / "soft" plaque), and produces a detailed structured report. Cleerly is a vendor name; HeartFlow, Elucid, and others are in the same space. When patients say "Cleerly scan" they usually mean a CCTA with the AI layer.
If your calcium score came back positive
Many people reading this are holding one specific result: a coronary calcium score that came back above zero. Here is how I read it.
First, what it is not. A positive calcium score is not a heart attack, not an emergency, and not a reason for the emergency room in the absence of symptoms. It is a risk marker: proof that atherosclerosis has already started, and a rough measure of how much. That is worth knowing precisely because it is actionable while you feel completely well.
The number sorts roughly into bands: 1 to 99 is mild plaque, 100 to 399 is moderate, 400 and above is extensive. Just as important is the age-and-sex percentile. A score of 50 is reassuring at 70 and concerning at 45, because it means plaque is accumulating faster than it should. A younger person with any positive score at all has arteries that are aging ahead of schedule.
What a positive score should change: it reclassifies your risk upward, and for most patients that tips the decision toward starting or intensifying preventive therapy. A positive calcium score is one of the strongest reasons to begin a statin in someone who was previously on the fence, and to treat to a stricter LDL goal (often under 70 mg/dL) rather than a casual one. Blood pressure, blood sugar, Lp(a), and lifestyle all get pulled into the same tighter frame.
The trap I see most often is the reassuring shrug: a patient gets a positive score, is told "you have a little calcium, we'll keep an eye on it," and leaves with no change in treatment. A positive score is established coronary disease. "Keep an eye on it" without lowering the LDL that is driving it is not a plan.
When a positive score leads to a CCTA: if you also have symptoms that could be cardiac (exertional chest pressure, breathlessness), or the score is very high, a CCTA can show whether any of that plaque is actually limiting blood flow and needs more than medication. For an asymptomatic positive score, though, the answer is usually to treat, not to keep imaging. And a calcium score is not a monitoring tool the way LDL or ApoB is: on effective treatment the calcium number can even rise as soft plaque stabilizes into denser calcified plaque, so a higher score on a repeat scan is not treatment failure. We track the lipids, not the calcium, to know whether therapy is working.
The patients who benefit from CCTA
In my practice, CCTA is most useful in two clear scenarios and one narrower third.
1. Stable, possibly-cardiac chest discomfort, no known coronary disease, middle-aged. The classic case: a 50-year-old with intermittent chest pressure that may be exertional, family history of heart disease, otherwise reasonably healthy, intermediate-range risk on the calculator. Pretest probability of coronary artery disease is high enough to take seriously but not so high that we are going straight to invasive testing.
CCTA answers a question stress tests struggle with: is there coronary plaque, even if it is not yet causing reduced blood flow? A stress test looks at whether blood flow is impaired. If an artery is 60% blocked and still letting blood through, a stress test will say "no ischemia" and you walk out reassured. That can be misleading. A CCTA would show that 60% blockage directly.
2. Asymptomatic, borderline risk, reluctant to start a cholesterol-lowering medication, where the result would change the decision. Someone in their late 40s, LDL is borderline, 10-year risk is moderate, they want to wait on a statin. A CCTA showing meaningful plaque is often the thing that flips the decision. A clean CCTA is reassuring and reasonable to act on. Either result changes what we do, which is the test of whether the test was worth ordering.
3. Patients with inflammatory or metabolic conditions (lupus / SLE, rheumatoid arthritis, HIV, type 2 diabetes) where standard risk calculators systematically underestimate cardiac risk. A patient I see often: a 53-year-old woman with SLE and chest pressure that is sometimes exertional, LDL 150, reluctant to start a statin. SLE roughly doubles or triples her cardiac risk beyond what the calculator estimates. CCTA is the right test for that patient, and if it shows non-obstructive plaque, which it often does, that is the motivating result to start aggressive prevention.
The patients who don't need one
Plenty of patients who ask about a Cleerly scan do not need one.
- Symptoms that suggest acute coronary syndrome (sudden severe chest pain, prolonged, at rest, with sweating or nausea). That is an emergency department visit, not a scan request. CCTA is for stable patients.
- Very low risk: young, no family history, normal lipids, no symptoms. CCTA will not find anything meaningful and exposes you to contrast and radiation for no decision change.
- Already known high-risk patient on optimal therapy. If you have established coronary disease, are already on a high-intensity statin, blood pressure is controlled, and you are not having symptoms, a CCTA is not going to change management.
- Heavy calcification expected (older patient, prior calcium score above ~400). Dense calcium scatters the X-rays and makes artery walls look more blocked than they are. In that scenario, a different test is usually better.
- Severe kidney disease or contrast allergy. Contrast dye is required and may not be safe.
- Atrial fibrillation or persistently fast / irregular heart rate. The CT relies on a slow, regular rhythm. If you cannot take a beta blocker to slow your heart, image quality drops a lot.
The question I ask before ordering one: "Will the result of this scan actually change something: start a medication, refer for invasive evaluation, or genuinely reassure?" If I cannot articulate "if positive we will do X, if negative we will do Y," the test is not earning its place.
Cleerly's added layer
The AI overlay does two things plain CCTA does not easily provide.
Plaque composition. It distinguishes calcified plaque (more stable, lower acute risk) from low-attenuation / "soft" plaque (more prone to rupture and cause heart attacks). Two patients with the same total plaque can have very different acute risk depending on composition.
Quantification. It produces a number you can track over time: total plaque volume, percent stenosis per vessel, composition breakdown. Done manually this is tedious; AI makes it routine.
Whether that quantification actually changes management is the real question. For most patients with non-obstructive disease the prescription is the same: aggressive statin, blood-pressure control, LDL goal under 70 mg/dL. Knowing whether plaque is 30% soft versus 50% soft does not usually change what is prescribed.
Where the quantification does earn its keep: as a motivator for patients who are reluctant about preventive therapy. "You have meaningful soft plaque in your left anterior descending artery" lands very differently than "you have some plaque." For patients who need a concrete picture of what is at stake, that is worth something.
Acting on the result
This is where I see the most variation in patient experience. A common pattern: patient gets the scan, gets a long report with terms they do not understand, has a brief follow-up where the conclusion is "looks fine, keep doing what you are doing," even when "fine" actually means "has measurable non-obstructive disease that warrants treatment intensification."
| Result | What it means | What we should do |
|---|---|---|
| Normal coronaries | No plaque seen. | Reassure. Look elsewhere for the symptom. Continue baseline prevention. |
| Non-obstructive plaque | Some plaque, no significant narrowing. | This is coronary artery disease. Intensify prevention: statin to a stricter LDL goal (typically <70), blood pressure control, address smoking or diabetes. The plaque is real even though it is not yet blocking flow. |
| 40–90% stenosis | Moderate-to-severe narrowing in one or more vessels. | FFR-CT (a flow calculation from the same images) can tell us whether the narrowing is actually reducing blood flow. If yes, consider stress testing or invasive evaluation. Optimize medical therapy regardless. |
| Left main ≥50% or severe 3-vessel disease | High-risk anatomic disease. | Cardiology evaluation, typically invasive. Do not manage as routine outpatient follow-up. |
The biggest interpretive trap is the second row: non- obstructive plaque. Reports often read benignly ("no obstructive coronary artery disease"), but what they actually mean is "CAD without significant blockage," which is still CAD, and still warrants more aggressive prevention than someone with truly clean arteries.
Practical considerations
Cost. Out-of-pocket CCTA runs $500–1500 depending on the imaging center and whether AI quantification is added. Some insurance covers it with appropriate indication; some does not. Ask up front.
Where to get it done. Image quality matters. Newer scanners with proper protocols make a real difference in reliability. If you are paying out-of-pocket, ask about scanner generation and protocol.
Who reads the result. A CCTA report from a radiologist not familiar with how cardiologists actually use the result can leave you with more confusion than clarity. The interpretation — what this means for your care, what to start, what to monitor, when to retest — is the part that matters.
Have Cleerly or CCTA results you want walked through?
Book a Video Visit